How Do You Reduce Healthcare Staff Turnover?
· 7 min read
You reduce healthcare staff turnover by screening nurses and clinical staff for reliability, communication, and stress tolerance before the offer, then moving them through fast, compliant, documented onboarding. Roughly half of frontline leavers quit inside their first 90 days, before competency sign-off, and replacing one frontline healthcare worker costs $5,000-$20,000, with SHRM putting skilled-role replacement at 50-200% of salary. The phone screen most units still rely on is close to a coin flip, tracking real ward performance at about ~0.18, whereas a structured interview paired with validated assessments carries the signal past 0.6, so tightening that screen is the highest-leverage retention fix you have.
Why is healthcare staff turnover so costly?
Healthcare staff turnover is so costly because every empty clinical seat is paid for twice, once in agency premiums and overtime to cover the gap, and again in the recruiting and onboarding spend to replace the person. Unlike a desk role, a nursing or clinical vacancy cannot simply wait; the shift still has to be staffed, so the bill starts the day someone leaves, not the day you finish hiring.
The pattern is the same one that drives employee turnover everywhere, only amplified by regulation and round-the-clock coverage. A candidate who looked fine on a resume but cannot carry the pace, the documentation burden, or the emotional load of patient care leaves fast, and in healthcare you absorb credentialing, orientation, and competency sign-off before you ever recover that investment. The 90-day cliff here is not just a screening miss; it is a screening miss on a seat you were legally and ethically required to keep filled.
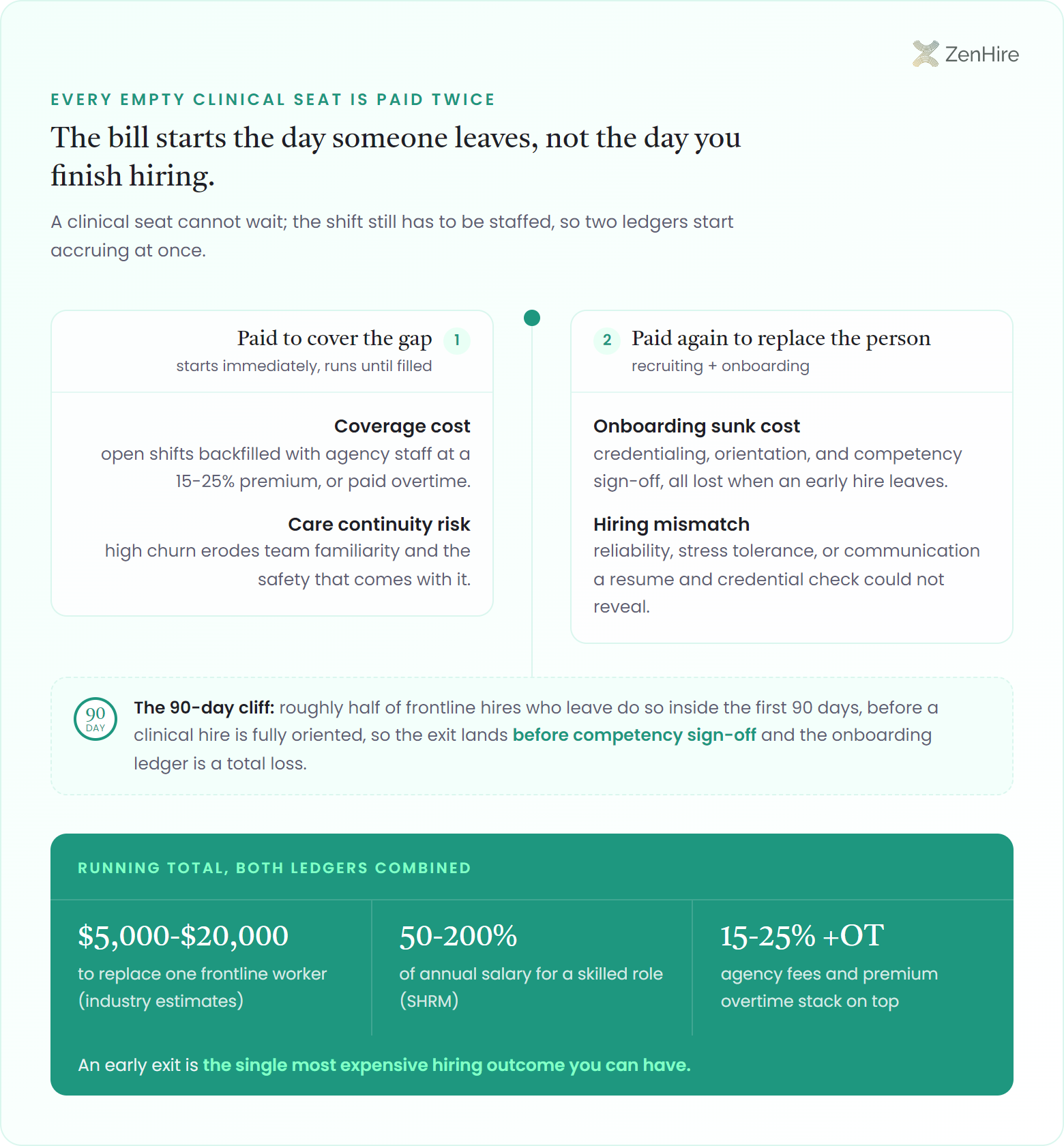
Roughly half of frontline hires who leave do so inside the first 90 days (before a clinical hire is fully oriented), and replacing one frontline worker runs $5,000-$20,000 (industry estimates), with SHRM putting skilled-role replacement at 50-200% of annual salary. In healthcare, agency placement fees of 15-25% and premium overtime to cover open shifts stack on top, so an early exit is the single most expensive hiring outcome you can have.
- Coverage cost: open shifts get backfilled with agency staff at a 15-25% premium or paid overtime
- Onboarding sunk cost: credentialing, orientation, and competency sign-off are lost when an early hire leaves
- Care continuity risk: high churn erodes team familiarity and the safety that comes with it
- Hiring mismatch: reliability, stress tolerance, or communication a resume and credential check could not reveal
How do you hire healthcare staff for fit and tenure?
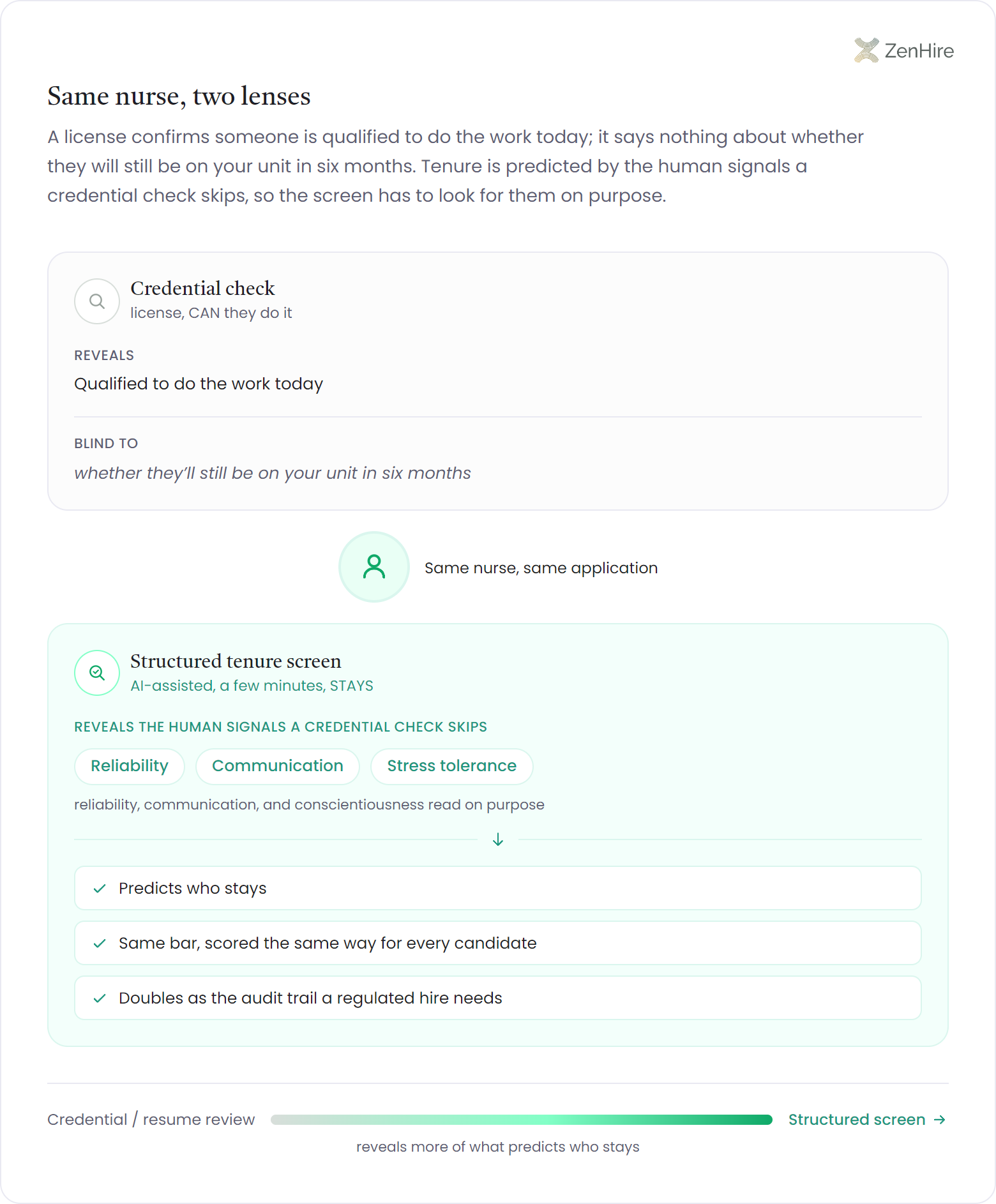
You hire healthcare staff for fit and tenure by evaluating reliability, communication, and stress tolerance consistently before the offer, not just verifying credentials. A license confirms someone is qualified to do the work; it says nothing about whether they will still be on your unit in six months. Tenure is predicted by the human signals a credential check skips, so the screen has to look for them on purpose.
Structured, AI-assisted screening adds the two things a stretched nurse manager or clinical recruiter cannot maintain by hand: consistency and scale. Every candidate clears the same bar, scored the same way, so a strong communicator is not lost because they applied during a staffing crunch. A structured interview reads communication, conscientiousness, and reliability signals in a few minutes, and the same evidence is on file whether you are filling one charge-nurse role or staffing an entire new wing. This is what lifts your quality of hire without adding steps a busy unit cannot sustain. Because the evaluation is the same for everyone, it also doubles as the audit trail a regulated hire needs.
Where you spend the screening effort matters more than how much you spend: reading a resume and verifying a license lands around r = 0.14 for predicting ward performance, and a chat-style interview only nudges it to ~0.18, while a structured interview backed by cognitive and skills assessments lifts the combined signal past 0.6, more than four times the predictive power, which is the gap between a nurse who ramps to competency sign-off and one who is gone before it.
How do you speed compliant healthcare hiring?
You speed compliant healthcare hiring by making the screen itself fast, consistent, and fully documented, so cutting time-to-fill never means cutting the paper trail a regulated hire requires. In most clinical pipelines the delay is not the credential check; it is the inconsistent, manual front end where strong candidates wait days for a first screen and the candidate experience sends them elsewhere. Standardize that step and you reclaim the time without touching compliance. The same discipline that shortens time to hire is what keeps quality high while you move faster.
A glass-box, structured assessment shortens the front of the funnel and strengthens the back of it at once. Because the interview is audio-only and runs about four minutes, an applicant who applies between shifts can finish it on a break and have a scored evaluation the same day, while the explainable scorecard and auditable decision log are exactly what a fairness review or labor audit asks for. ZenHire's AI interview software is SOC 2 and GDPR aligned and excludes demographic factors by design, so faster screening and defensible, reduced-bias hiring are the same motion, and you can track the payoff directly in time-to-hire.
| What you standardize | What it buys a healthcare team |
|---|---|
| Same-day structured screen | Fewer drop-offs: strong clinical candidates are scored before a competitor reaches them |
| Explainable scorecards | An audit-ready record of why each hire cleared the bar |
| Demographic factors excluded | Defensible, reduced-bias screening under regulatory scrutiny |
| SOC 2 + GDPR posture | Candidate data handled to the standard a clinical employer is held to |

In healthcare everyone optimizes the credential check and ignores the screen, which is backwards. A license tells you someone can legally do the job; it tells you nothing about whether they will still be on the ward in three months. I have watched hospitals lose good hires not because the credentialing was slow but because the human screen in front of it was a coin flip; strong candidates waited days for an inconsistent phone interview and took the offer that moved first. The fix is not to lower the bar to go faster. It is to make the bar identical for everyone, scored in minutes, and written down. That is the only way I know to hire faster and survive an audit at the same time.
Frequently asked questions
Why is healthcare staff turnover so expensive?+
Healthcare staff turnover is so expensive because an empty clinical seat is paid for twice: agency premiums of 15-25% or overtime to cover the open shift, plus the recruiting and onboarding spend to replace the person. Replacing one frontline worker runs about $5,000-$20,000 (industry estimates), and SHRM puts skilled-role replacement at 50-200% of salary.
How do you improve nurse retention through hiring?+
You improve nurse retention by screening for reliability, communication, and stress tolerance before the offer, not just verifying credentials. A license confirms qualification but not tenure; the human signals that predict who stays on a unit are caught in a structured, consistent screen, which is also far more predictive than an unstructured interview.
Can you hire healthcare staff faster without breaking compliance?+
Yes: faster hiring and compliance are the same motion when the screen is structured and documented. A glass-box, explainable assessment gives every candidate a same-day scored evaluation while producing the auditable decision log a regulated hire requires, so you shorten time-to-fill without thinning the paper trail.
What is the biggest cause of early healthcare turnover?+
The biggest cause of early healthcare turnover is hiring mismatch: a candidate who cleared the credential check but could not carry the pace, documentation load, or emotional weight of patient care. It shows up as the 90-day cliff, where industry studies put roughly half of leavers gone before they are fully oriented.
Does AI screening introduce bias risk in clinical hiring?+
Structured AI screening can lower bias risk relative to inconsistent manual screening when it is explainable and excludes demographic factors. A glass-box system aligned to SOC 2 and GDPR scores every candidate the same way and keeps an auditable log, which is more defensible under scrutiny than undocumented human judgment.
Free for reducing healthcare staff turnover
The healthcare retention hiring checklist
A one-page checklist for cutting early clinical turnover at the hire: the reliability and communication signals to weight for nursing and frontline staff, plus the documentation that keeps a fast pipeline audit-ready.